
Diagnostic
Clinique & ECG
– Douleur angineuse continue et récente (plus de 15 minutes)
– ECG :
- Sus décalage de ST dans 2 dérivations adjacentes > 0.1mV dans les standards > 0.2mV dans les précordiales
- images en miroir
- Sous décalage de ST dans 2 dérivations adjacentes
- ECG normal
– douleur trinitro-résistante
consultez le simulateur ECG

Importance de l’anamnèse
– ATCD personnels, terrain, facteurs de risque cardiovasculaire, circonstances de survenue
– Rechercher un diabète, une insuffisance rénale (facteurs de gravité).
Diagnostics différentiels
– péricardite, myocardite, dissection aortique, embolie pulmonaire, intoxication digitalique, intoxication au CO...
BILAN PARACLINIQUE
Bilan de routine
– ECG 18 dérivations (à renouveler)
– Glycémie capillaire
– Monitorage Scope, PNI, SpO2
Bilan spécifique
– Hémostase (Groupe, NFS, plaquettes, TP, TCA)
– Myoglobine + Troponine (en cas de ST+ ne pas attendre les résultats pour entreprendre la recanalisation d’urgence).
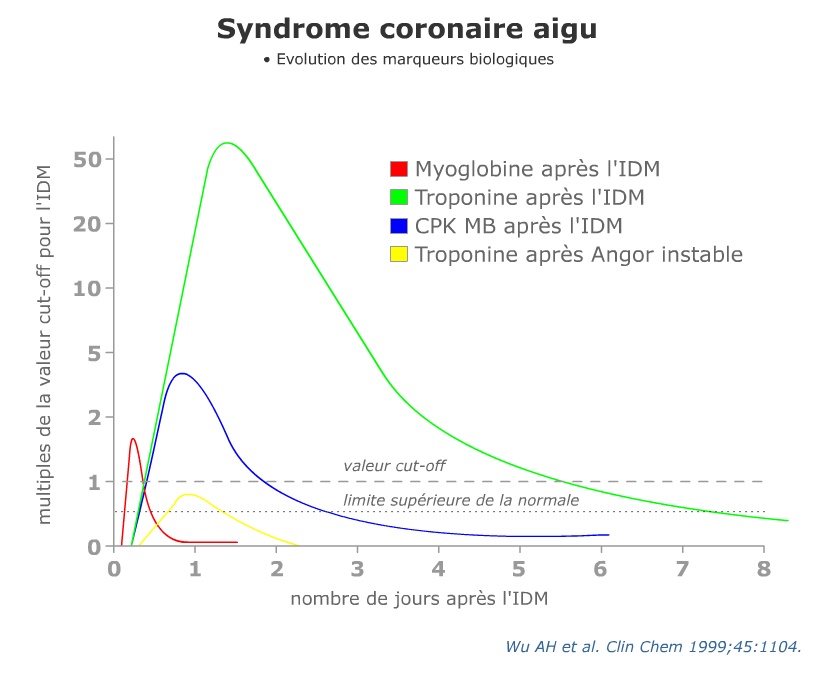
La troponine s’élève entre la quatrième et la sixième heure. Répéter le prélèvement +++
Interprétation des résultats de la Troponine T ultra sensible
– TnTc HS <0,014 ng/mL :
- et douleur thoracique > 3h
- sortie avec discussion des explorations ambulatoires à 30 jours
- et douleur thoracique < 3h
- répéter le dosage 3 heures après le premier prélèvement
- augmentation <0,007 ng/mL ou <30%, sortie avec discussion des explorations ambulatoires à 30 jours
- augmentation >0,007 ng/mL ou >30%, discuter avec le cardiologue de l’admission pour explorations.
- répéter le dosage 3 heures après le premier prélèvement
– TnTc HS 0,014-0,05 ng/L :
- répéter le dosage 3 heures après le premier prélèvement
- augmentation <0,007 ng/mL ou <30%, sortie avec discussion des explorations ambulatoires à 30 jours
- augmentation >0,007 ng/mL ou >30%, discuter avec le cardiologue de l’admission pour explorations.
– TnTc HS >0,05 ng/mL :
- discuter avec le cardiologue de l’admission pour explorations.
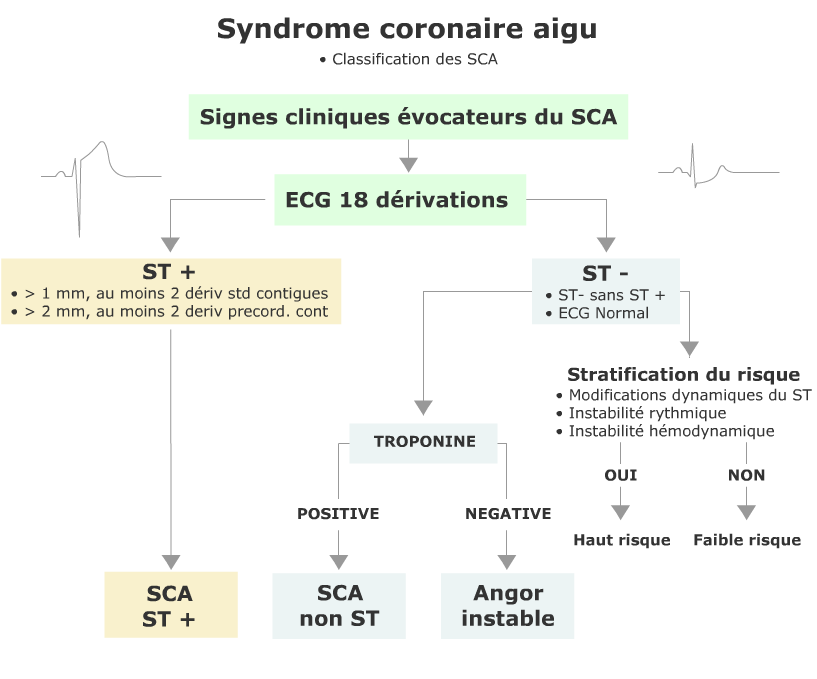
Classification des SCA
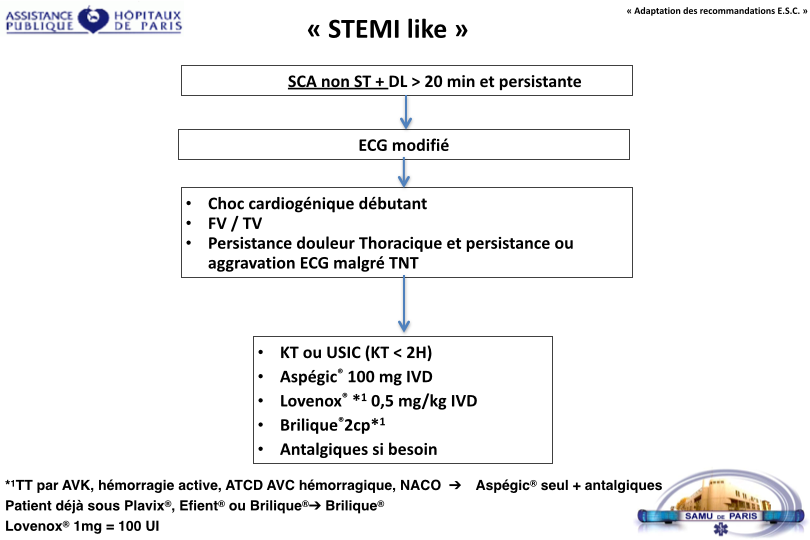
TRAITEMENT
Thérapeutique symptomatique
– Test aux dérivés nitrés. L’usage intra veineux est limité aux SCA non ST (en respectant les contre indications) et en surveillant étroitement la PA la fonction ventriculaire droite.
– Morphine titrée (en fonction de l’EVS) , anxiolytiques éventuels.
– 2 voies veineuses (G5% et Nacl) en garde veine.
– O2 si spo2 < 93% ou Killip > 1
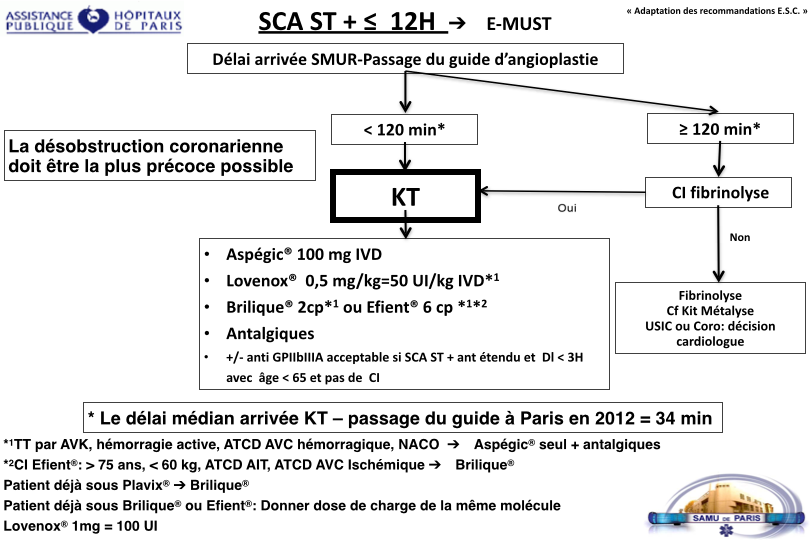
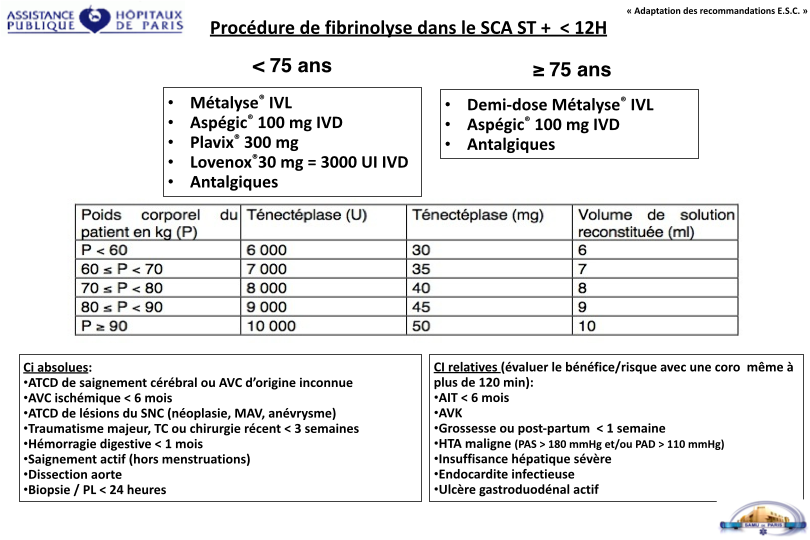
Thérapeutique spécifique
Protocole officiel du SAMU de PARIS, SMUR Necker, SMUR Hôtel Dieu, SMUR Lariboisiere, SMUR Pitié.


Rappels de pharmacologie :
| Nom | Classe | Action | Administration |
|---|---|---|---|
| Clopidogrel (Plavix®) | anti-adhésif et anti-agrégant plaquettaire de la classe des thiénopyridines antagoniste irréversible du récepteur P2Y à l’ADP, ce qui empêche l’activation du complexe GPIIb-IIIa. |
Délai d’action : 2h Pic : 6h Durée d’action : 7-10 jours (durée de vie des plaquettes) |
per os |
| Ticagrelor (Brilique®) | anti-adhésif et anti-agrégant plaquettaire de la classe des cyclopentyltriazolopyrimidines antagoniste sélectif et réversible du P2Y, n’agissant pas au site d’action de l’ADP, mais empêchant la transduction du signal. |
Délai d’action : < 30 min Pic : 2-4h Durée d’action : 4 jours |
per os |
| Prasugrel (Efient®) | anti-adhésif et anti-agrégant plaquettaire de la classe des thiénopyridines antagoniste irréversible du récepteur P2Y à l’ADP, ce qui empêche l’activation du complexe GPIIb-IIIa. |
Délai d’action : < 30 min Pic : 4h Durée d’action : 7-10 jours (durée de vie des plaquettes) |
per os |

TIMI Score Risk pour le SCA non ST
| --- Facteur de risque --- | --- Points --- | --- Mortalité à J 14 --- |
|---|---|---|
| à‚ge >= 65 ans | 1 | 5% |
| > 3 facteurs de risque coronaire | 1 | 8% |
| Cardiopathie ischémique reconnue | 1 | 13% |
| prise d’aspirine au cours des 7 derniers jours | 1 | 20% |
| Douleur angineuse récente | 1 | 26% |
| Augmentation des enzymes | 1 | 41% |
| Sous décalage de ST > 0,5 mm | 1 | - |
Score de risque = Total des points (0-7)
– Classification ESC
| Patient à haut risque | Patients à faible risque |
|---|---|
| douleurs thoraciques récidivantes et/ou modifications dynamiques du ST | pas de douleur thoracique au cours de la période d’observation |
| modifications du segment ST non interprétables | ST normal mais T<0 ou plates |
| élévation du taux de troponine | |
| troponine normale | |
| instabilité hémodynamique | |
| arythmies majeures TV/FV | |
| diabète type 1 | |
| angor instable précoce après IDM |
– Calculateurs de risque
Références
– Acute coronary syndromes, Scottish Intercollegiate Guidelines Network - SIGN (Feb 2013)
– Steg G, James S et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation European Heart Journal (2012) 33, 2569&2619
– Scheuermeyer FX, Innes G, Grafstein E, et al. Safety and Efficiency of a Chest Pain Diagnostic Algorithm With Selective Outpatient Stress Testing for Emergency Department Patients With Potential Ischemic Chest Pain. Ann Emerg Med. Jan 4 2012 ;
– Hamm CW, Bassand JP, Agewall S, et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation : The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. Sep 21 2011
– Hyperglycaemia in acute coronary syndromes, NICE Clinical Guideline (October 2011)
– Acute coronary syndromes - ticagrelor, NICE Technology Appraisal Guideline (October 2011)
– Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Hlatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes : a meta-analysis. J Am Coll Cardiol. Aug 2001 ;38(2):478-85.
– O’Connor RE, Bossaert L, Arntz HR, Brooks SC, Diercks D, Feitosa-Filho G, et al. Part 9 : acute coronary syndromes : 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. Oct 19 2010 ;122(16 Suppl 2):S422-65.
– Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Hlatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes : a meta-analysis. J Am Coll Cardiol. Aug 2001 ;38(2):478-85.
– Chest pain of recent onset, NICE Clinical Guideline (March 2010)
– Unstable angina and NSTEMI, NICE Clinical Guideline (March 2010)
– Swanson N, Montalescot G, Eagle KA, et al ; Delay to angiography and outcomes following presentation with high-risk, Heart. 2009 Mar ;95(3):211-5. Epub 2008 Sep 18.
– Acute coronary syndrome - prasugrel, NICE Technology Appraisal Guideline (October 2009)
– Peters RJ, Mehta S, Yusuf S ; Acute coronary syndromes without ST segment elevation. BMJ. 2007 Jun 16 ;334(7606):1265-9.
– Cohen M, Diez JE, Levine GN, et al ; Pharmacoinvasive management of acute coronary syndrome : incorporating the 2007 ACC/AHA guidelines : the CATH (cardiac catheterization and antithrombotic therapy in the hospital) Clinical Consensus Panel Report—III. J Invasive Cardiol. 2007 Dec ;19(12):525-38 ; quiz 539-40.
– Conway Morris A, Caesar D, Gray S, et al ; TIMI risk score accurately risk stratifies patients with undifferentiated chest pain presenting to an emergency department. Heart. 2006 Sep ;92(9):1333-4.
– Sabatine MS, Morrow DA, Giugliano RP, et al ; Implications of upstream glycoprotein IIb/IIIa inhibition and coronary artery stenting in the invasive management of unstable angina/non-ST-elevation myocardial infarction : a comparison of the Thrombolysis In Myocardial Infarction (TIMI) IIIB trial and the Treat angina with Aggrastat and determine Cost of Therapy with Invasive or Conservative Strategy (TACTICS)-TIMI 18 trial. Circulation. 2004 Feb 24 ;109(7):874-80. Epub 2004 Feb 2.
– Lagerqvist B, Husted S, Kontny F, et al ; A long-term perspective on the protective effects of an early invasive strategy in unstable coronary artery disease : two-year follow-up of the FRISC-II invasive study. J Am Coll Cardiol. 2002 Dec 4 ;40(11):1902-14.
– Culic V, Eterovic D, Miric D, et al ; Symptom presentation of acute myocardial infarction : influence of sex, age, and risk factors. Am Heart J. 2002 Dec ;144(6):1012-7.
– Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined—a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. Sep 2000 ;36(3):959-69.
– Antman EM, Tanasijevic MJ, Thompson B, Schactman M, McCabe CH, Cannon CP, et al. Cardiac-specific troponin I levels to predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med. Oct 31 1996 ;335(18):1342-9.
– Heidenreich PA, Alloggiamento T, Melsop K, McDonald KM, Go AS, Hlatky MA. The prognostic value of troponin in patients with non-ST elevation acute coronary syndromes : a meta-analysis. J Am Coll Cardiol. Aug 2001 ;38(2):478-85.
– GRACE ; Global Registry of Acute Cardiac Events
– The TIMI Study Group
Nous informons nos visiteurs que Urgences-Serveur.fr n'est pas un service médical, ni une téléconsultation.
Aucun conseil ni avis médical ne sera donné via ce forum.
Consultez votre médecin si vous pensez être malade.
Composez le 15 en cas d'urgence médicale.
Vos commentaires
Pour participer à ce forum, vous devez vous enregistrer au préalable. Merci d’indiquer ci-dessous l’identifiant personnel qui vous a été fourni. Si vous n’êtes pas enregistré, vous devez vous inscrire.
Suivre les commentaires : |
|
